Matters of the Heart
 As they age, men and women differ in one of the most significant aspects of life—matters of the heart. No, not the emotional side of the heart, but the physical side of heart health. For many women in the United States, menopause presents a range of recognized symptoms including hot flashes, weight gain, mood swings, and vaginal pain and dryness on intercourse. These changes can affect quality of life but seldom are lethal. More insidious are risks of breast cancer and osteoporosis. Yet, heart disease is THE leading cause of death among women in America.
As they age, men and women differ in one of the most significant aspects of life—matters of the heart. No, not the emotional side of the heart, but the physical side of heart health. For many women in the United States, menopause presents a range of recognized symptoms including hot flashes, weight gain, mood swings, and vaginal pain and dryness on intercourse. These changes can affect quality of life but seldom are lethal. More insidious are risks of breast cancer and osteoporosis. Yet, heart disease is THE leading cause of death among women in America.
Common early symptoms of heart disease are more subtle for women than those for men. The classic male presentation is pain along the left arm and jaw coupled with tightening and pain in the chest. These recognized symptoms are likely to initiate an emergency room visit, immediate cardiac evaluation, and likelihood of coronary angiography with possible stent placement or coronary bypass surgery. For women, the early symptom of heart disease most frequently seen is unusual fatigue, but some women experience sleep disorders, shortness of breath, indigestion, anxiety, and even rarely, chest discomfort. These complaints are dismissed easily as reflecting the stresses of everyday life. The vague nature of these complaints helps explain the reduced use of cardiac evaluations when women present with these symptoms. Healthcare providers need to have a high index of suspicion when evaluating women with fatigue and/or these other symptoms to consider cardiac disease after ruling out anemia, thyroid disease, depression, and anxiety along with other more rare disorders.
The biologic differences in heart disease between men and women help explain the contrasting symptoms. For men, a heart attack is preceded by a series of biologic events in which oxidized cholesterol damages the endothelial cells lining the coronary arteries. These damaged cells draw immune cells from the blood into the coronary artery wall where they help develop into a space occupying plaque which can lead to compromised blood flow. If and when this plaque finally ruptures, a thrombus (clot) blocks the artery leading to cardiac muscle damage and possible death. For women, presumably due to the unique hormonal environment, only tiny lipid plaques form and are distributed throughout the smaller coronary blood vessels, which probably explains the more subtle symptoms of women's heart disease.
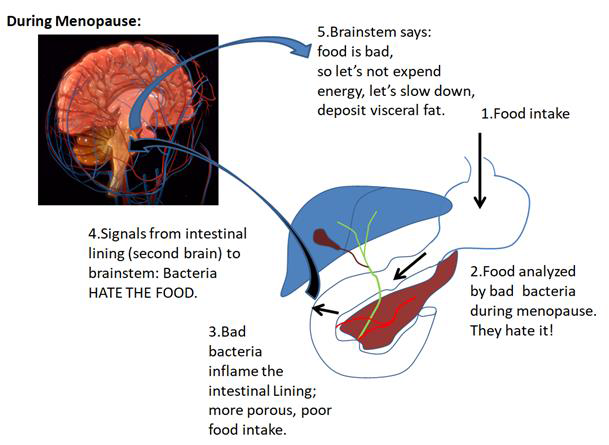
Both family history and lifestyle contribute to defining a person's risk of heart disease. A strong family history increases risk, and that component of heart health is non‐preventable. In contrast, we can control many lifestyle factors. Smoking is the leading modifiable risk factor linked to heart disease, yet obesity is not far behind. Estimates are that two‐thirds of menopausal women are overweight or obese, and with obesity comes increased insulin resistance and a heightened risk of diabetes. While our subcutaneous (SQ) fat is esthetically unpleasant, it is the visceral fat (around our organs and inside our abdomen) that produces many of the inflammatory proteins linked to heart disease. Moreover, visceral fat cells also exist as a thin fat layer lying directly on our blood vessels, thereby giving their inflammatory proteins direct access to our circulation. Fortunately, studies have shown that weight loss efforts (diet and exercise) can reduce both SQ and visceral fat.
While women's heart health may seem complex, we have made significant advances in educating both providers and women regarding identifying at‐risk groups and early diagnosis of heart disease. There is now more emphasis than ever on preventive and predictive measures in women's heart health with the hope of decreasing heart disease as the leading killer of women.
By James Woods, M.D.
Dr. Woods treats patients for menopause at the Hess/Woods Gynecology Practice.
Disclaimer: The information included on this site is for general educational purposes only. It is not intended nor implied to be a substitute for or form of patient specific medical advice and cannot be used for clinical management of specific patients. Our responses to questions submitted are based solely on information provided by the submitting institution. No information has been obtained from any actual patient, and no physician-patient relationship is intended or implied by our response. This site is for general information purposes only. Practitioners seeking guidance regarding the management of any actual patient should consult with another practitioner willing and able to provide patient specific advice. Our response should also not be relied upon for legal defense, and does not imply any agreement on our part to act in a legal defense capacity.
James Woods | 5/26/2015